SARS-CoV-2 と COVID-19 に関するメモ・備忘録
佐藤佳・東大教授が率いるG2P-Japanチームから、変異株BA.2.86(ピロラ)に続いてEG.5(エリス)の解析に関する論文が出されました。
佐藤研からはこれまで数々の研究成果が論文で発表されていて世界の医療に貢献しているのですが、お膝元の日本政府(永田町&霞ヶ関)が政策にまったく活かしていないのはホンマなんなんでしょうね・・・
#拡散希望 速報🔔 G2P-Japan🇯🇵の論文第27弾「新型コロナ変異株EG.5とXBBブレイクスルー感染の関連解析」を、Lancet Infectious Diseases @TheLancetInfDis に発表しました。本研究では、世界で流行拡大中の #オミクロン EG.5(俗称 #エリス)の特性を解明しました。1/https://t.co/EAciwKhhss
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
最近、XBB.1.9の亜系統「EG.5(XBB.1.9.2.5)」の感染拡大が、国内外(のツイッター/X)で話題になっています。特にEG.5.1は、XBB.1.9.2(スパイクはXBB.1.5と同じ)のスパイクに、#Q52H と #F456L というふたつの変異が追加されたものです。2/https://t.co/s4iOkJq9vN pic.twitter.com/7yKbTxFPSD
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
EG.5の流行拡大は、ようやく日本でも報道され始めました。ちなみに、#WHO は8月9日に(ひと月前の時点ですでに)、この株を、現状最高ランクの「variant of interest(注目すべき変異株)」に分類しています。3/https://t.co/ls5TvykJhN
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
本研究ではまず、@jampei2 による流行動態解析によって、EG.5.1の相対的な実効再生産数(Re)は、日本を含む複数の国において、XBB.1.5よりも約1.2倍ほど大きいことを明らかにしました。つまりEG.5.1は、次の主流な株となるポテンシャルを持っている株と言えます。4/ pic.twitter.com/T6xFhtatiw
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
次に、シュードウイルスを用いた実験をしましたが、EG.5.1の感染力価は、XBB.1.5/1.9.2より若干低下していました。つまり、EG.5.1の高い実効再生産数(≒伝播力)は、感染力価の増大によるものではないことが示唆されます。5/ pic.twitter.com/ovj3GdJjjx
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
そして、XBB亜系統(XBB.1.5, XBB.1.9, XBB.1.16)のブレイクスルー感染の回復血清を用いた中和試験の結果、EG.5.1はは、XBB.1.5に比べて1.4倍の抵抗性を示しました。また、この抵抗性は、 #F456L 変異によって規定されていることも明らかにしました。6/ pic.twitter.com/3zDpzppEjD
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
つまり、EG.5.1の出現と流行は、XBB亜系統のブレイクスルー感染で獲得された免疫からの逃避によるものであると示唆されます。
※なお、この結果は、先発していたプレプリントの結果と異なりますが、これは解析に用いた検体数が増えたためです(8検体→24検体)。7/https://t.co/JkRs26uwx3
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
そして、重要な点として、XBB亜系統のブレイクスルー感染で誘導されたXBB亜系統に対する中和力価は、祖先株B.1.1の約6.3~6.6倍ほども低いことを見出しました。8/ pic.twitter.com/zQ2osIEM72
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
複数の先行研究で、オミクロンのブレイクスルー感染で誘導された、感染したオミクロン亜株(BA.1, BA.2, BA.5)に対する中和力価も、祖先株B.1.1に対するものよりも低いことが報告されていました。しかしそれらは、約2~3倍程度の低下に留まっていました。9/ pic.twitter.com/bUKkIpsQlU
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
つまり、XBB亜系統のブレイクスルー感染で誘導される中和抗体の力価は、過去のオミクロン亜株のブレイクスルー感染で誘導される力価よりも低いこと、そして、XBB亜系統のブレイクスルー感染では、高いレベルの液性免疫が誘導されない可能性があることが示唆されます。10/
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
ワクチンやその種類、感染履歴などなど、今や世界の人々の免疫バックグラウンドは多岐に富んでいます。このような集団としての複雑な免疫状態が、さまざまな変異株の同時出現や群雄割拠化、収斂進化の要因となっているのかもしれません。正直、まだまだわからないことだらけとも言えます…🎐11/
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
東大医科研 @Japanese_IMSUT からのプレスリリースはこちらから↓ 12/12https://t.co/z7Hbi4jnVh
— The Sato Lab (Kei Sato) (@SystemsVirology) September 12, 2023
◆Antiviral efficacy of the SARS-CoV-2 XBB breakthrough infection sera against omicron subvariants including EG.5【The Lancet 2023年9月11日】
The SARS-CoV-2 XBB lineage is a recombinant omicron lineage that emerged in the summer of 2022. As of July, 2023, some XBB sublineages bearing the F486P substitution in the spike protein (S; S:F486P), such as XBB.1.5 and XBB.1.16, have rapidly spread and become predominant in the world according to Nextstrain. Because S:F486P significantly increased pseudovirus infectivity, it is assumed that the spread of F486P-bearing XBB subvariants is attributed by the increased infectivity by S:F486P.
As of July, 2023, EG.5.1 (also known as XBB.1.9.2.5.1), a XBB subvariant bearing the S:Q52H and S:F456L substitutions, alongside the S:F486P substitution, has rapidly spread in some Asian and North American countries. On Aug 9, 2023, WHO classified EG.5 as a variant of interest. In fact, our epidemic dynamics analyses showed that EG.5.1 exhibits a higher effective reproduction number (Re) compared with XBB.1.5, XBB.1.16, and its parental lineage (XBB.1.9.2), suggesting that EG.5.1 will spread globally and outcompete these XBB subvariants in the near future.
To assess the possibility that the enhanced infectivity of EG.5.1 contributes to its augmented Re, we prepared the lentivirus-based pseudoviruses with the S proteins of XBB.1.5/1.9.2 (note that the XBB.1.5 S is identical to the XBB.1.9.2 S), EG.5.1, and two XBB.1.5/1.9.2 derivatives, XBB.1.5/1.9.2+Q52H and XBB.1.5/1.9.2+F456L. The pseudovirus assay showed that both S:Q52H and S:F456L did not increase pseudovirus infectivity, and the pseudovirus infectivity of EG.5.1 was significantly lower than that of its parental lineage (XBB.1.9.2). These results suggest that the increased Re is not due to the increased infectivity caused by these substitutions.
We then performed a neutralisation assay using XBB breakthrough infection (BTI) sera (n=24) to address whether EG.5.1 evades the antiviral effect of the humoral immunity induced by BTI of XBB subvariants. As shown on appendix p 13, the 50% neutralisation titre (NT50) of XBB BTI sera against EG.5.1 was significantly (1·4-fold) lower than those against the parental XBB.1.5/1.9.2 (p<0·0001). The NT50 values of XBB BTI sera against XBB.1.5/1.9.2, XBB.1.16, and XBB.1.5/1.9.2+Q52H were comparable. However, the NT50 value of XBB BTI sera against XBB.1.5/1.9.2+F456L was significantly (1·9-fold) lower than that of the parental XBB.1.5/1.9.2 (p<0·0001, appendix p 13). These results suggest that the increased Re of EG.5.1 is partly attributed to the immune evasion from the humoral immunity elicited by XBB BTI, and S:F456L is a key mutation leading to this immune evasion. We previously demonstrated that omicron BTI cannot efficiently induce antiviral humoral immunity against the infecting variant. In fact, the NT50values of the BTI sera of omicron BA.1, BA.2, and BA.5 against the infecting variant were 3·0-fold, 2·2-fold, and 3·4-fold lower than that against the ancestral B.1.1 variant, respectively. Strikingly, however, we found that the NT50 value of the BTI sera of XBB1.5/1.9.2 and XBB.1.16 against the infecting variant were 6·6-fold and 6·3-fold lower than that against the B.1.1 variant. These results suggest that the BTI of XBB subvariants cannot efficiently induce antiviral humoral immunity against the infecting variants when compared with the BTI of previous omicron variants.
This work was supported in part by the Japan Agency for Medical Research and Development (AMED) Strategic Center of Biomedical Advanced Vaccine Research and Development for Preparedness and Response (SCARDA) Japan Initiative for World-leading Vaccine Research and Development Centers UTOPIA programme (JP223fa627001 to KSat); AMED SCARDA Program on R&D of New Generation Vaccine Including New Modality Application (JP223fa727002 to KSat); AMED Research Program on Emerging and Re-emerging Infectious Diseases (JP22fk0108146 to KSat; JP21fk0108494 to G2P-Japan Consortium and KSat; JP21fk0108425 to KSat; JP21fk0108432 to KSat; JP22fk0108511 to G2P-Japan Consortium and KSat; JP22fk0108516 to KSat; JP22fk0108506 to KSat); AMED Research Program on HIV/AIDS (JP22fk0410039 to KSat); Japan Science and Technology Agency (JST) Precursory Research for Embryonic Science and Technology (PRESTO; JPMJPR22R1 to JI); JST Core Research for Evolutional Science and Technology (CREST; JPMJCR20H4, to KSat); Japan Society for the Promotion of Science (JSPS) KAKENHI Grant-in-Aid for Early-Career Scientists (23K14526 to JI); JSPS Core-to-Core Program (A Advanced Research Networks; JPJSCCA20190008 to KSat); JSPS Research Fellow DC2 (22J11578 to KU); JSPS Research Fellow DC1 (23KJ0710 to YKo); The Tokyo Biochemical Research Foundation (to KSat); and The Mitsubishi Foundation (to KSat). JI has received consulting fees and honoraria for lectures from Takeda Pharmaceutical. KSat has received consulting fees from Moderna Japan and Takeda Pharmaceutical and honoraria for lectures from Gilead Sciences, Moderna Japan, and Shionogi & Co. All other authors declare no competing interests. YKa, YKo, KU, and JI contributed equally to this study. Members of The Genotype to Phenotype Japan (G2P-Japan) Consortium are listed in the appendix (p 15).
流石にど素人の俺でもおかしいってわかるよ。だって発症してから3日以内に処方するべき薬を、発症してから3日間以上の自宅療養求めた後に投薬しましょうとか言ってるわけで。検査→治療(投薬)という海外で普通にやってる手順の中身が、なんでこんなに雑になるのか。 https://t.co/g1ME3jpEYI
— ガイチ (@gaitifuji) September 17, 2023
教条が事実に優先するためです。
— Hiroshi Makita Ph.D. 誰が日本のコロナ禍を悪化させたのか?扶桑社8/18発売中 (@BB45_Colorado) September 17, 2023
オミクロン株への対応には日本は完全に失敗していて、日本の300%は過小評価と推定される死亡統計ですら合衆国と同じ最悪グループに入っています。(中進国以上は精々50%程度の過小評価。)
韓国は、大統領選の時の緩和で大勢死にましたが、その後は持ち直しています。
— Hiroshi Makita Ph.D. 誰が日本のコロナ禍を悪化させたのか?扶桑社8/18発売中 (@BB45_Colorado) September 17, 2023
新型コロナウイルス感染症の感染過程で自然呼吸中に吐き出される 1 分あたりの SARS-CoV-2 RNA コピーの量を示す、この貴重な研究で気になったところを軽く見ていきたいと思います。
私が気になったのはどれだけウイルスを排出してるかなんですよね。https://t.co/jH6golkAm5
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
新型コロナに感染した人が日数経過とともにどれくらい呼気にウイルスを排出しているか。
1000コピー近く出してる人がそこそこいるなと気づきます、少ない数ではないなと。8日目以降の減少は認められるかなといった感じです。
5日では無理です、まぁ5日は無根拠な数字なので無意味なんですけどね。 pic.twitter.com/FITrObtj07— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
さて、ちょっと気になったのはここ。
感染成立に必要なウイルスの個数を控えめに3000億個としてます。そして、900コピーを叩き出す人はどれくらいで感染成立する個数のウイルスを吐き出すか。
20秒で3000億個のウイルスを出します。
一秒で150億個です、一分で9000億個、一時間で54兆個。— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
54兆個なんて新型コロナのウイルス量をノーマスクで吐き出されたらアウトです。
では一番マイルドなパターンの30分で3000億個を呼気に吐き出す場合では、一秒で1.67億個。
一時間で6000億個を超えます、換気が不十分な場所では簡単に感染成立しますね。さて、賢い人なら分かるやついきます。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
このウイルス排出量を不織布マスクでどれくらいガードできるかを示す研究やデータがあるので見たら分かるのですが、プリーツ型マスクを着用した場合に漏れ率が30%でも一時間で1800億個程度までは抑えることができます。
呼気の側が着用するのがポイント。ノーマスクだと全部出て、全部吸います。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
感染している側が不織布のプリーツ型マスクをして一時間に1800億個程度まで落としたウイルス量を、今度は換気や空気清浄で減らしていきます。
では、ここでCDCが推奨する一時間に5回の換気をHEPAフィルターの空気清浄機で行ったとします。
12分に一度空気が入れ替わる計算ですね。— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
一番マイルドなパターンの呼気へのウイルス排出量は12分で1202.4億個となりました。
ここにHEPAフィルターの粒子捕捉率を99.97%としますと……36億ちょっとだけ残ります。
実際にやると分かりますがHEPAフィルターの捕捉率はエグいのでほぼほぼ0までもってけます。
おや、これは……
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
マイルドなパターンならマスク着用と1時間で5回の換気や空気清浄を組み合わせると感染成立する個数まで空間にウイルスが溜まりませんね。
これがスイスチーズモデルなんです。
もちろんこれは空間に感染者が一人でマイルドな場合での想定ですが、このように考えれば良い訳ですね。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
また一番エグいパターンでも12分で1800億個なので、ここでマスク着用して換気や空気清浄機をやれば感染成立個数に到達するのは防げる計算になります。
スイスチーズモデルがわかればこんな感じですね。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
一番エグいパターンでも不織布のプリーツマスクで漏れ率が30%でも12分に一度の換気、空気清浄をすれば540億個で止まります。
ここでしっかり換気や空気清浄をすれば感染を止められる算段がつきます。感染していると症状が出る前からウイルスを排出する、症状に気づかなくてもウイルスを呼気に出す。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
この呼気に含まれるウイルス排出量を踏まえると「厚労省が言ったからマスク着用はしたい人がやればいい」は、あまりに乱暴な思考停止という事が分かるでしょう。
マスクしたくないと言う考えはは簡単に相手を感染させてしまうウイルス量を出してしまうことがデータで示された証左の一つですね。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
JR、特に新幹線やバス車内で換気や空気清浄が不完全であると非常に怖いことが分かるでしょう。
このウイルス量が空間に満ちるとアウトなんです、ゆえに呼気をそのまま出すノーマスクは本当に愚策なんです。3000億個と言う個数は相当緩い計算なのでもっと少なくても感染成立するのでシビアーですね。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
ここでマスクプラスの「その空間で一時間に5回換気するには、どれくらいの風量(空気清浄機の風量)が必要か」も出しておきましょう。
このツールにはお世話になってます。https://t.co/RGLOJeljPu
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
例えば六畳間は室面積が約10㎡、日本の家屋は大体高さが2.4メートルだそうなのでこれを入れて一時間の換気回数を入れます。
もし、六畳間で家庭内感染を止めるよう隔離するなら、これくらいの風量で綺麗な空気を吐き出す空気清浄機やコルジ・ローゼンタールボックスが欲しいです。 pic.twitter.com/k70WWCGEmp
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
ちなみに日本版コルジ・ローゼンタールボックスとも言えるクレアウィンボックスはこのボックスに50cmほどのボックスファンを組み合わせたものです。
この風量はざっと計算したんですが1000㎥/hを軽く超えます。
計算したら日本家屋で50畳に対応しました(凄い)https://t.co/LK5pBJT2Bm
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
学校の教室の広さから考えると一個で足りますね、ただしノーマスクではない前程ですが。
今や学校はちょっと文科省もどうかしてるし教育委員会もどうかしてるしでマスク一枚まともにできない有様。
コルジ・ローゼンタールボックスだけで飛沫対策は無理。
さらに出されるウイルス量がエグいです。 pic.twitter.com/5uOEaAhsdt— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
と、理詰めしていくと「マスク外すのがいかに非効率的か分かる」のと「そりゃノーマスクがウロついてたら感染する」のと「マスクと一緒に換気や空気清浄噛ませたら十分使えるね」と言う話でした。
丼ぶり勘定ではなく、こうやって理詰めするんですよ。
予防の人は丼ぶり勘定なんて絶対しません。— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
……で、新型コロナの病態が長期障害がエグすぎるわ、と言う知見があればマスクくらいしますよ。
感染対策するのは「合ってます」
極めて「合理的」だし「理性的」感染対策しっかりやる人は褒めちゃいます、と答え合わせにもなるのでした。
空気清浄を嫌う理由?
分かりませんね!
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
と、言う訳で「適切な知見を組み合わせること」が大切です。
今度は飛沫の飛散距離を見ます、ノーマスクの会話で1.5mは出ますね。ちなみに声が大きくなれば、もっと飛散距離は遠くなります。
誰だい?1.5m離れてるから科学的だとドヤっていたのは予防原則知らんのか。https://t.co/tbuzp7eMFQ pic.twitter.com/RXJkmKw86y— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
そして、前述の飛沫とエアロゾルは屋内では拡散されるはずもないです。
特にエアロゾルは滞留します、有名な論文を。新型コロナウイルスことSARS-CoV-2が実験期間の3時間はエアロゾルとして滞留して生きてます、エアロゾルとして出されたら思いっきり感染しますね。https://t.co/NOlOyixT2W pic.twitter.com/FRTFEQ0HUa
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
屋内、及び覆いや壁など遮蔽物がある屋外ではエアロゾルが滞留してしまいます。
また前述の歩行やすれ違いだけでも感染者からのエアロゾルは喰らってます。自転車ならマスク外してもいい、は、ちょっとその点ではよろしくないです。
街中では無防備にウイルス暴露を重ねる可能性が高い。— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
はい、理詰め理詰め。
新型コロナに感染して「大したことない」なんてのは正常性バイアスのそれです。natureのこの論文はよくまとまってるので見ると良いです、どんだけの症状や病態が新型コロナウイルスで引き起こされるのかを理解しておくこと。
分かったフリはダメ。https://t.co/Tv59v54Uob pic.twitter.com/N9lH03XJ6G
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
そんな訳である程度の知見はこのスレッドで見られるようにしました。
ウイルス曝露量が少ないほど症状が軽い、と言うのは研究であったので尚更感染対策はしておきたいですね。
「治せない物があまりに多い病気を確実に予防する」のは安価かつ最適な生存戦略でしょう、賢い人のやり方です。
— うじー@感染対策魔人はマスク着用と科学で対処 (@medical_for_all) September 18, 2023
◆Quantity of SARS-CoV-2 RNA copies exhaled per minute during natural breathing over the course of COVID-19 infection【medRxiv 2023年9月8日】
ABSTRACT
SARS-CoV-2 is spread through exhaled breath of infected individuals. A fundamental question in understanding transmission of SARS-CoV-2 is how much virus an individual is exhaling into the environment while they breathe, over the course of their infection. Research on viral load dynamics during COVID-19 infection has focused on internal swab specimens, which provide a measure of viral loads inside the respiratory tract, but not on breath. Therefore, the dynamics of viral shedding on exhaled breath over the course of infection are poorly understood. Here, we collected exhaled breath specimens from COVID-19 patients and used RTq-PCR to show that numbers of exhaled SARS-CoV-2 RNA copies during COVID-19 infection do not decrease significantly until day 8 from symptom-onset. COVID-19-positive participants exhaled an average of 80 SARS-CoV-2 viral RNA copies per minute during the first 8 days of infection, with significant variability both between and within individuals, including spikes over 800 copies a minute in some patients. After day 8, there was a steep drop to levels nearing the limit of detection, persisting for up to 20 days. We further found that levels of exhaled viral RNA increased with self-rated symptom-severity, though individual variation was high. Levels of exhaled viral RNA did not differ across age, sex, time of day, vaccination status or viral variant. Our data provide a fine-grained, direct measure of the number of SARS-CoV-2 viral copies exhaled per minute during natural breathing—including 312 breath specimens collected multiple times daily over the course of infection—in order to fill an important gap in our understanding of the time course of exhaled viral loads in COVID-19.
INTRODUCTION
SARS-CoV-2, the causative agent of COVID-19, spreads through exhaled breath during coughing, talking, singing, and breathing. Levels of SARS-CoV-2 over the course of infection have been extensively characterized in upper and lower respiratory tract specimens such as nasopharyngeal and oropharyngeal swabs, whereas the dynamics of levels on breath over the course of infection remain virtually unexplored. This is despite the fact that quantifying levels of viral shedding on exhaled breath would allow for a direct approximation of the amount of virus an individual is shedding into the environment, thereby exposing others to risk of infection. We know particularly little about the dynamics of viral shedding on breath during unlabored natural breathing, which serves as a baseline for viral transmission on breath.
While the dynamics of viral load inside the host respiratory tract has direct relevance to viral pathology, dynamics of viral load on the host’s breath has direct relevance to infectiousness. Understanding the dynamics of viral shedding on breath is important for prevention of transmission of disease. Measuring viral load characteristics of the primary route of onward transmission is critical to inform isolation times in the clinic, where isolation consumes scarce resources, and to inform public health transmission control protocols. In addition, variables that impact level of viral shedding on breath remain unclear, but may vary by a multitude of factors including symptom severity, days since symptom onset, co-morbidities, viral genotype, and other unknowns. Understanding of these factors requires quantification of exhaled viral loads, which cannot be inferred from internal viral loads.
Current techniques for measuring viral load in exhaled breath have successfully detected SARS-CoV-2 in specimens, though with variable detection rates ranging from 26.9% to 86%. Recent work has also shown that SARS-CoV-2 can be isolated from exhaled breath, confirming that it contains replication-competent virus. However, prior work has focused on exertive breathing conditions (talking, singing, coughing), and we therefore have less understanding of viral loads in exhaled breath during natural breathing. Furthermore, prior work has not analyzed exhaled breath collected longitudinally over the course of infection relative to the day of symptom onset (potentially due to expense and lack of portability of breath collection devices), which would allow for a better understanding of the time course of changes in viral loads on breath. An inexpensive, portable device that allows patients to self-collect breath samples at home would facilitate research into factors that contribute to virus transmission from breath, how exhaled virus levels change over the course of infection, and whether therapeutics and other interventions reduce levels of exhaled virus.
Here, we developed a portable, disposable exhaled breath condensate collection device (EBCD) (Fig S1) and used it to collect 312 specimens from 60 COVID-19-tested outpatients who were treated at Northwestern Memorial Hospital (NMH). Specimens were analyzed using RT-qPCR. Our data set included breath specimens collected multiple times per day over the course of infection. We report numbers of SARS-CoV-2 RNA copies exhaled per minute, during natural breathing, over the course of infection and across a range of factors including self-reported symptom severity, age, sex, presence of co-morbidities, vaccination status and viral variant.
◆Long COVID: major findings, mechanisms and recommendations【nature:nature reviews microbiology 2023年1月13日】
Abstract
Long COVID is an often debilitating illness that occurs in at least 10% of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections. More than 200 symptoms have been identified with impacts on multiple organ systems. At least 65 million individuals worldwide are estimated to have long COVID, with cases increasing daily. Biomedical research has made substantial progress in identifying various pathophysiological changes and risk factors and in characterizing the illness; further, similarities with other viral-onset illnesses such as myalgic encephalomyelitis/chronic fatigue syndrome and postural orthostatic tachycardia syndrome have laid the groundwork for research in the field. In this Review, we explore the current literature and highlight key findings, the overlap with other conditions, the variable onset of symptoms, long COVID in children and the impact of vaccinations. Although these key findings are critical to understanding long COVID, current diagnostic and treatment options are insufficient, and clinical trials must be prioritized that address leading hypotheses. Additionally, to strengthen long COVID research, future studies must account for biases and SARS-CoV-2 testing issues, build on viral-onset research, be inclusive of marginalized populations and meaningfully engage patients throughout the research process.
Introduction
Long COVID (sometimes referred to as ‘post-acute sequelae of COVID-19’) is a multisystemic condition comprising often severe symptoms that follow a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. At least 65 million individuals around the world have long COVID, based on a conservative estimated incidence of 10% of infected people and more than 651 million documented COVID-19 cases worldwide; the number is likely much higher due to many undocumented cases. The incidence is estimated at 10–30% of non-hospitalized cases, 50–70% of hospitalized cases and 10–12% of vaccinated cases. Long COVID is associated with all ages and acute phase disease severities, with the highest percentage of diagnoses between the ages of 36 and 50 years, and most long COVID cases are in non-hospitalized patients with a mild acute illness, as this population represents the majority of overall COVID-19 cases. There are many research challenges, as outlined in this Review, and many open questions, particularly relating to pathophysiology, effective treatments and risk factors.
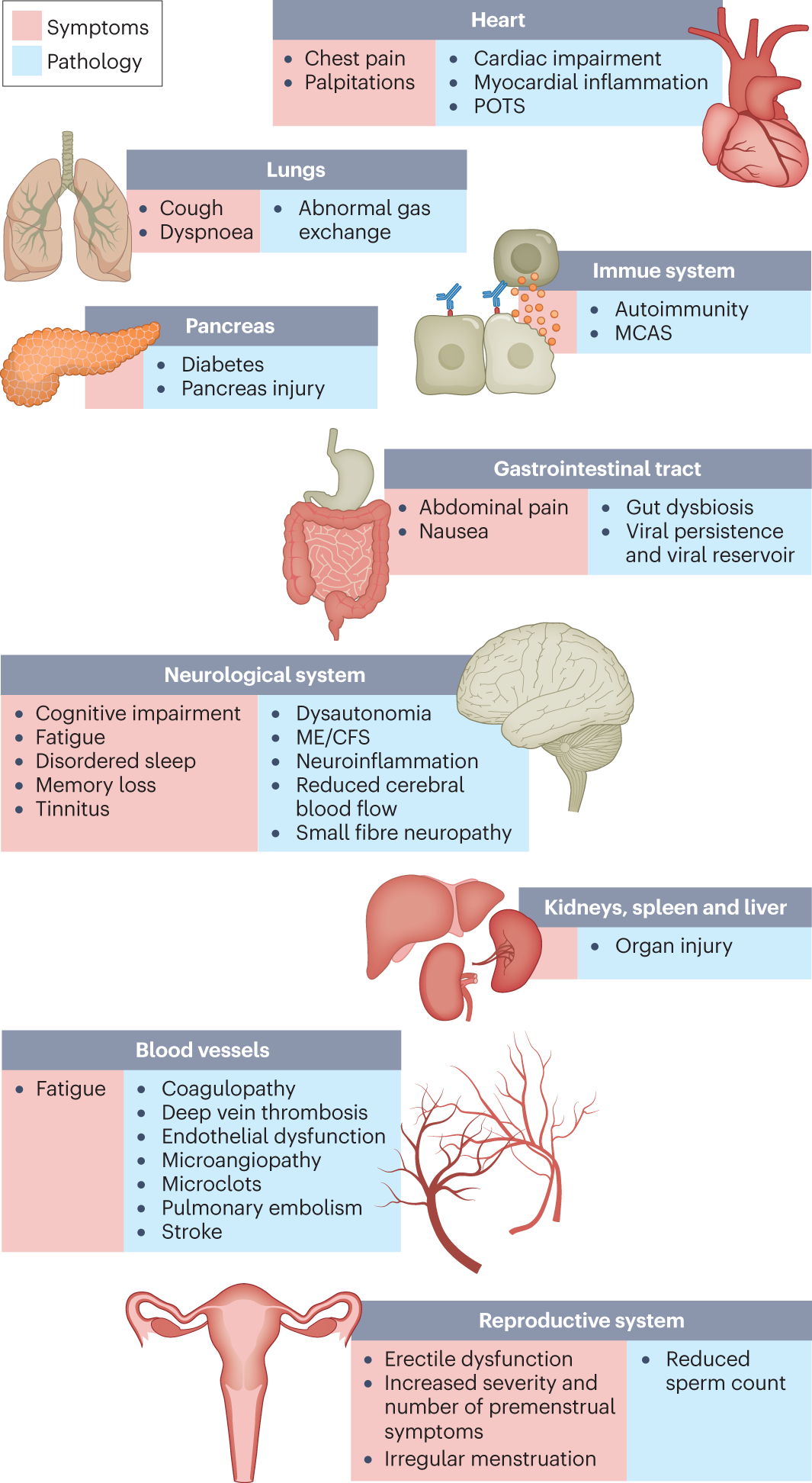
Hundreds of biomedical findings have been documented, with many patients experiencing dozens of symptoms across multiple organ systems (Fig. 1). Long COVID encompasses multiple adverse outcomes, with common new-onset conditions including cardiovascular, thrombotic and cerebrovascular disease, type 2 diabetes, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and dysautonomia, especially postural orthostatic tachycardia syndrome (POTS) (Fig. 2). Symptoms can last for years, and particularly in cases of new-onset ME/CFS and dysautonomia are expected to be lifelong. With significant proportions of individuals with long COVID unable to return to work7, the scale of newly disabled individuals is contributing to labour shortages. There are currently no validated effective treatments.
Fig. 1: Long COVID symptoms and the impacts on numerous organs with differing pathology.
The impacts of long COVID on numerous organs with a wide variety of pathology are shown. The presentation of pathologies is often overlapping, which can exacerbate management challenges. MCAS, mast cell activation syndrome; ME/CFS, myalgic encephalomyelitis/chronic fatigue syndrome; POTS, postural orthostatic tachycardia syndrome.Fig. 2: SARS-CoV-2 infection, COVID-19 and long COVID increases the risk of several medical conditions.
Because diagnosis-specific data on large populations with long COVID are sparse, outcomes from general infections are included and a large proportion of medical conditions are expected to result from long COVID, although the precise proportion cannot be determined. One year after the initial infection, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections increased the risk of cardiac arrest, death, diabetes, heart failure, pulmonary embolism and stroke, as studied with use of US Department of Veterans Affairs databases. Additionally, there is clear increased risk of developing myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and dysautonomia. Six months after breakthrough infection, increased risks were observed for cardiovascular conditions, coagulation and haematological conditions, death, fatigue, neurological conditions and pulmonary conditions in the same cohort. The hazard ratio is the ratio of how often an event occurs in one group relative to another; in this case people who have had COVID-19 compared with those who have not. Data sources are as follows: diabetes, cardiovascular outcomes, dysautonomia, ME/CFS and breakthrough infections.There are likely multiple, potentially overlapping, causes of long COVID. Several hypotheses for its pathogenesis have been suggested, including persisting reservoirs of SARS-CoV-2 in tissues; immune dysregulation with or without reactivation of underlying pathogens, including herpesviruses such as Epstein–Barr virus (EBV) and human herpesvirus 6 (HHV-6) among others; impacts of SARS-CoV-2 on the microbiota, including the virome; autoimmunity and priming of the immune system from molecular mimicry; microvascular blood clotting with endothelial dysfunction; and dysfunctional signalling in the brainstem and/or vagus nerve (Fig. 3). Mechanistic studies are generally at an early stage, and although work that builds on existing research from postviral illnesses such as ME/CFS has advanced some theories, many questions remain and are a priority to address. Risk factors potentially include female sex, type 2 diabetes, EBV reactivation, the presence of specific autoantibodies, connective tissue disorders, attention deficit hyperactivity disorder, chronic urticaria and allergic rhinitis, although a third of people with long COVID have no identified pre-existing conditions6. A higher prevalence of long Covid has been reported in certain ethnicities, including people with Hispanic or Latino heritage. Socio-economic risk factors include lower income and an inability to adequately rest in the early weeks after developing COVID-19. Before the emergence of SARS-CoV-2, multiple viral and bacterial infections were known to cause postinfectious illnesses such as ME/CFS, and there are indications that long COVID shares their mechanistic and phenotypic characteristics. Further, dysautonomia has been observed in other postviral illnesses and is frequently observed in long COVID.
Fig. 3: Hypothesized mechanisms of long COVID pathogenesis.
There are several hypothesized mechanisms for long COVID pathogenesis, including immune dysregulation, microbiota disruption, autoimmunity, clotting and endothelial abnormality, and dysfunctional neurological signalling. EBV, Epstein–Barr virus; HHV-6, human herpesvirus 6; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.In this Review, we explore the current knowledge base of long COVID as well as misconceptions surrounding long COVID and areas where additional research is needed. Because most patients with long COVID were not hospitalized for their initial SARS-CoV-2 infection, we focus on research that includes patients with mild acute COVID-19 (meaning not hospitalized and without evidence of respiratory disease). Most of the studies we discuss refer to adults, except for those in Box 1.
Box 1 Long COVID in children
Long COVID impacts children of all ages. One study found that fatigue, headache, dizziness, dyspnoea, chest pain, dysosmia, dysgeusia, reduced appetite, concentration difficulties, memory issues, mental exhaustion, physical exhaustion and sleep issues were more common in individuals with long COVID aged 15–19 years compared with controls of the same age. A nationwide study in Denmark comparing children with a positive PCR test result with control individuals found that the former had a higher chance of reporting at least one symptom lasting more than 2 months. Similarly to adults with long COVID, children with long COVID experience fatigue, postexertional malaise, cognitive dysfunction, memory loss, headaches, orthostatic intolerance, sleep difficulty and shortness of breath. Liver injury has been recorded in children who were not hospitalized during acute severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections, and although rare, children who had COVID-19 have increased risks of acute pulmonary embolism, myocarditis and cardiomyopathy, venous thromboembolic events, acute and unspecified renal failure, and type 1 diabetes. Infants born to women who had COVID-19 during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first year after delivery. A paediatric long COVID centre’s experience treating patients suggests that adolescents with a moderate to severe form of long COVID have features consistent with myalgic encephalomyelitis/chronic fatigue syndrome. Children experiencing long COVID have hypometabolism in the brain similar to the patterns found in adults with long COVID. Long-term pulmonary dysfunction is found in children with long COVID and those who have recovered from COVID-19. Children with long COVID were more likely to have had attention deficit hyperactivity disorder, chronic urticaria and allergic rhinitis before being infected.
More research on long COVID in children is needed, although there are difficulties in ensuring a proper control group due to testing issues. Several studies have found that children infected with SARS-CoV-2 are considerably less likely to have a positive PCR test result than adults despite seroconverting weeks later, with up to 90% of cases being missed. Additionally, children are much less likely to seroconvert and, if they develop antibodies, are more likely to have a waning response months after infection compared with adults.


Scandinavian Journal of Work, Environment & Health「重症COVID-19疾患やSARS-CoV-2感染と関連する職業的リスク – 2020年10月~2021年12月に実施されたスウェーデン全国症例対照研究」 https://t.co/vnENlQjFLx
重症感染リスクが高い職業はバスと路面電車の運転手、看護師、小学校教師、保育士と pic.twitter.com/qBg5nNWAOY— 森 勇一 (@ymori117) September 19, 2023
同じ運転手でもトラック運転手のリスクは上昇していない。つまり、不特定多数の乗客を乗せているかどうかが重要ってこと。
— 森 勇一 (@ymori117) September 19, 2023
で、中央省庁が、もともと重症感染リスクの高い小学校の先生からマスクを奪って、さらに大きな危険にさらす野蛮な国があるんです。日本ていう国なんですけど。
— 森 勇一 (@ymori117) September 19, 2023
コレ結構ほかでも似たような報告されてたし、僕の周りでもそう。公共交通機関の乗務員は物凄くリスク高い。ただ日本は列車が長いし、運転席は開放されてないので、電車はそこまででもないかも。やっぱり、一番目につくのは教師の被害。周りで唯一のLong covidも先生だし。子供の学校でも事情は不明だけど体調不良で結構昔からいる先生がいなくなったりしてるしね。いま学校で先生からマスクはずすみたいだけど、マジで大丈夫か?子供も心配だけど、小学校の特に女性教師はLong covidのHigh riskど真ん中なので、問題にならなければいいけど。あと業務命令ぽいのでちゃんとなんかあったときは補償して上げてほしい。 https://t.co/xkzberK5yK
— Kazz.MD.Ph.D. (@KazBowen) September 19, 2023
もちろんNurseはみんなわかってると思うので触れませんでした。医師よりリスク高かったよ。医師は科が違うとリスク全然違うから。看護師さんは基本入院患者さん見ること多いしね。接する時間が違うからね。本当に大変な仕事だと思う。特にひどいときは出征する兵士を送り出すようなCommunityの雰囲気だ…
— Kazz.MD.Ph.D. (@KazBowen) September 19, 2023
Long covid発症に関してはいくつか危険因子が確定していて、女性であることはかなり強い危険因子です。特に働ける年齢層は他の年齢層と比べてかなり発症のリスクが高いことが知られているからです。小学校の女の先生はその年代の人が多いかと思って。高齢者は逆にLong covidの相対リスクはひくいです
— Kazz.MD.Ph.D. (@KazBowen) September 19, 2023
はっきり言って、新型コロナウイルスを甘くみている連中による政治的な判断で決定された
・5日間の療養(5類化以後は推奨)
というルールが、悪法も法なりで学校の現場まで落ちていき、感染した生徒と周囲の生徒たちを苦しめているという現実には悲嘆せざるを得ない。
→— Offside🌻 (@yfuruse) September 20, 2023
中等症までいった生徒も5日間40度をこえる高熱にうなされた生徒も、発症日を0日として6日目に登校しないと欠席扱いにされる。そのタイミングで定期テストがあれば、救済案もなく無理に受けるしかない。そしてバリバリにウイルスを出している状態なのに、マスクをとれと言われる。
→— Offside🌻 (@yfuruse) September 20, 2023
高校生なら成績が悪くても大学受験でリカバリーができなくもないが、推薦入試では不利。中学生だと「内申重視」という入試制度の前に選択肢を狭められるし、私立高校の中には「中学3年間に10日以上の欠席がある子は合格しても入学を許可しない」というところもある。
→— Offside🌻 (@yfuruse) September 20, 2023
根本的な問題は
・感染症にかかるのも重篤化するのも本人の責任とは限らない
にもかかわらず
・欠席に対して非常に厳しい対応をする制度になっていること
である。つまり、「学校を休むような子は国家にとって役立たないから切り捨てろ」という制度になっているのに、誰もそれを疑わない。
→— Offside🌻 (@yfuruse) September 20, 2023
考えてみれば、ひどいいじめで登校できなくなった子への対応と共通している。いじめた子の登校を禁止するべきなのに、いじめられた子を放逐していく。
これはすなわち、いじめるような強い子は国の役にたつから全力で守るが、いじめられるような弱い子は役に立たないから切り捨てるというシステム
→— Offside🌻 (@yfuruse) September 20, 2023
「成績がのびなくても毎日学校にきている強い子には内申などで埋め合わせをするセーフティネットがある」というコメントをされた。
だったら「病気やいじめなどの理由で登校できない弱い子に対してもセーフティネットがあってしかるべき」でしょう。ましていまは未曾有の感染症が蔓延中だ。
→— Offside🌻 (@yfuruse) September 20, 2023
様々な研究結果をみるかぎり、新型コロナに感染すると14日間くらいはウイルスを吐出しているし、感染後90日間くらいは体内に炎症が残り、無理をすると憎悪する。発症日を0日として14日間は「欠席しても出席扱いにする」くらいの対応をして、生徒の健康回復を支援するべきじゃないか。切り捨てるな
→— Offside🌻 (@yfuruse) September 20, 2023
ともかく**いま**はウイルスと戦争中の非常時だ。なのに生徒の感染予防策を意図的に奪い、自分たちがマスクをとって積極的に生徒にうつし、感染した子が重い症状で苦しもうが6日目に出てこなかったら欠席扱い。そしてマスクもとらせ、すぐ部活の試合に出す。
この世の地獄が展開されている。— Offside🌻 (@yfuruse) September 20, 2023
そうです。津波警報の発令で一目散に丘へ逃げた生徒に「教室から抜け出して早退した」と叱るのかって話です。いまは
・生徒を感染させずに授業と行事を粛々とこなすこと
が最優先課題で、同時に
・感染した子が不利益を被ることなく、早く治癒するように配慮すること
が求められているはず。「リモートだと欠席扱いにするから、欠席日数がかさんで、希望の高校にはいけなくなるよ。ざまをみろ」という態度をとるべきではない。— Offside🌻 (@yfuruse) September 20, 2023
”平時”と”感染症流行時”の切り替えを言う学校衛生管理マニュアル。https://t.co/qOIcuHWEaM
切り替え判断は何を根拠に誰の責任で?
「マスクは個人の判断」と口出しつつ教育委員会や学校長の自立した判断を支持する文言なし。
国が”今は平時ではない”と宣言しない限り統制下の現場は”平時”に縛られる https://t.co/IljOl6fCct pic.twitter.com/n3WUN9FCa7— vogelsang7 (@vogelsang7) September 18, 2023
昨日静岡県教委に電話した。
県教委
>県の感染拡大警報は承知してます。
>流行時と判断するのは現場。判断の根拠(指標etc.)も指定なし。マスク着脱を「強いることのないように」すればマスク推奨、マスク着用を呼びかける教育的指導は自由。
>各学校のマスク指導は把握してません。自由です!
— vogelsang7 (@vogelsang7) September 19, 2023
上下関係で目上が呼びかければ下の者は”反抗”しづらくて、”強制”になってしまうんじゃ?と弱い立場へのケアからマスクへの言及すら遠慮する先生、それ間違い!
ELSI提言などでの「強制」の意味は、(欧米流の)倫理学・経済学での「強制の4段階」と「介入のはしご」で定義されていると考えるべき。
— vogelsang7 (@vogelsang7) September 19, 2023
従順な日本の子供相手ではなく、簡単に”反抗”してデモしたりストしたり自由で民主的な欧米の大人相手の「強制」が、ELSI提言などでの「強いる」の意味。
8段階の「介入のはしご」のうち、
①情報提供②(狭義の)ナッジ③インセンティブ④強制の4段階
を考え、④(レベル1,2)は「強制」。③は微妙? pic.twitter.com/XtpZ0ka9Kh— vogelsang7 (@vogelsang7) September 19, 2023
ぱっと検索して拾った適当なソースですが。https://t.co/v2hT7z4QB8https://t.co/QZkIqoumcX
— vogelsang7 (@vogelsang7) September 19, 2023
マスクなしの咳エチケットを”平時”の”基本”(デフォルト)とし、マスク推奨を”感染症流行時”の例外状態扱いする文科省のマニュアル自体、学校現場への”ナッジによる介入”として構築されている。
その誘導に乗るかは、学校現場の自由!
学校衛生管理マニュアル 2023/4/28 https://t.co/qOIcuHWEaM pic.twitter.com/KGI4IVFL5U
— vogelsang7 (@vogelsang7) September 19, 2023
で、けっきょく文科省から学校現場への”ナッジ”が、日本的な上下関係・権力構造の文脈では、ただのナッジで終わらなくて強制性を持ってしまうのではないか、現場の合理的な対応を阻害してしまうのでは、という問題に戻るよね。
文科省のナッジを振り払うために、現場の思慮と勇気と努力が要求される。
— vogelsang7 (@vogelsang7) September 19, 2023
ただのナッジが…。
国家が介入して市民社会の感染対策緩和を推進すべきとするELSI提言に呼応し、文科省は一転してノーマスクのデフォルト化を含むノーマスクへのナッジで構成されたマニュアルを発布。
ナッジの振り付けに忠誠競争する教員たちの掌返しが子供の信頼を裏切るhttps://t.co/5mULQQUCq1 pic.twitter.com/HQ0nFDQHwA— vogelsang7 (@vogelsang7) September 20, 2023
ちょっと待て
乗っかっていいのか
そのナッジ感染症流行期やぞ。
— vogelsang7 (@vogelsang7) September 20, 2023
昼、文科省初等中等教育健康教育・食育課に「学校衛生管理マニュアル」について電話しました。
文科省
>文科省や教育委員会が「平時」か「感染症流行時」かの判断を示すことはしません。現場・個人の主体的判断が尊重されます。
>校長が「平時」か「感染症流行時」か判断して学校としての……— vogelsang7 (@vogelsang7) September 21, 2023
>…取り組みを切り替えるのは現場の自由です。
>学校としての判断とは別に、生徒職員個人が”今は感染症流行時だ”と独自に判断して自分のマスク着用の方針を主体的に判断することも尊重されます。私:個人が「今は平時」と判断して平時の感染対策メニューを選ぶのと「今は感染症流行時」と……
— vogelsang7 (@vogelsang7) September 21, 2023
…判断して感染症流行時の感染対策メニューを選ぶのは、どちらも尊重されるんですね。
文科省>その通りです。私:マニュアルには「平時」の感染対策メニューを大きく目立たせて扱い、「感染症流行時」のメニューを小さく扱っているが、個人や学校がどちらのメニューを選ぶとしても……
— vogelsang7 (@vogelsang7) September 21, 2023
…その選択の判断を尊重する、ということですね。
文科省>そうです。私:このマニュアルは専門用語ではリバタリアン・パターナリズムのナッジにもとづく選択メニューだと思いますが、省内でそういう議論があったのですか?
文科省>別にそういう専門用語では議論していません。
……— vogelsang7 (@vogelsang7) September 21, 2023
…
私:学校現場がこういう選択メニューの提示になれていなくて、「平時」のデフォルトとされた「マスクしない」状態を実現しようと努力してしまう、マニュアルのデフォルトへの忠誠競争のような状況が一部で見られますが、文科省の意図ではないんですね。
文科省>文科省の意図ではありません。
….— vogelsang7 (@vogelsang7) September 21, 2023
私:文科省からこういう選択メニューの提示は、あまり前例がないと思います。文科省の意図が現場に伝わらず一部では「デフォルト・メニュー」への忠誠競争のようになっているようです。意図が明確に伝わるような取り組みをお願いします。
文科省>ご意見を承りました。
やりとりは以上。
— vogelsang7 (@vogelsang7) September 21, 2023
なるほど。二重、三重の解釈を許す「学校衛生管理マニュアル」のテキストの多義性は、批判の矛先をたらい回しにしてそれぞれのアクターが批判をかわしながら現場を”コロナ明け”演出に誘導していく”最適解”なんだな。https://t.co/c68u3kdW0g
— vogelsang7 (@vogelsang7) September 22, 2023